19/12/2021
Published in
Microbioblog and The Conversation
Ignacio López-Goñi
Full Professor of Microbiology, University of Navarra
 Omicron sounds like an apocalypse. The WHO has decided to name the different variants following the Greek alphabet: Alpha: B.1.1.7; Beta: B.1.351; Gamma: P.1; Delta: B.1.617.2; Epsilon: B.1.427/B.1.429; Zeta: P.2; Eta: B.1.525; Theta: P.3; Lota: B.1.526; Kappa: B.1.617.1; Lambda: C.37; Mu: B.1.621. The next in the list was supposed to be Nu, but as it sounded like "New"(new) decided to move on to the next one, Xi. But it turns out that the Chinese president is called Xi JinPing and it was better not to touch his nose. The next letter of the alphabet was Omicron. So the new variant B.1.1.529 is called Omicron. And with Omicron came chaos.
Omicron sounds like an apocalypse. The WHO has decided to name the different variants following the Greek alphabet: Alpha: B.1.1.7; Beta: B.1.351; Gamma: P.1; Delta: B.1.617.2; Epsilon: B.1.427/B.1.429; Zeta: P.2; Eta: B.1.525; Theta: P.3; Lota: B.1.526; Kappa: B.1.617.1; Lambda: C.37; Mu: B.1.621. The next in the list was supposed to be Nu, but as it sounded like "New"(new) decided to move on to the next one, Xi. But it turns out that the Chinese president is called Xi JinPing and it was better not to touch his nose. The next letter of the alphabet was Omicron. So the new variant B.1.1.529 is called Omicron. And with Omicron came chaos.
In times of widespread pandemic fatigue it is essential to remember that fear on speech does not usually work. We have seen this with climate change: doom and gloom messages end up boring and many people switch off, as in the children's story of Peter and the wolf (I am not referring to Sánchez).
We have been receiving apocalyptic messages for months: "English variant of COVID-19 would be 64% more deadly according to a study", "This is the dangerous South African variant that is already in Asturias", "Brazilian variant, twice as contagious and capable of reinfecting up to 60%", "An expert warns about the Californian strain: the devil is already here".
Once again, with Omicron, it is time for rigour, transparency (saying what we know and what we don't know) and, above all, proposing solutions.
Omicron is much more transmissible
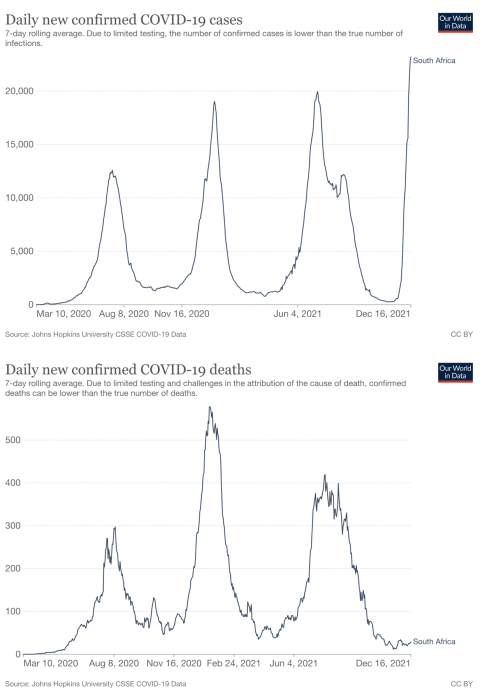
Since it was detected a few weeks ago, it has been spreading intensively in many countries. It seems that its growth is skyrocketing, exponential, and that in a few weeks it will displace the hitherto dominant Delta variant. However, although it is still too early to tell, some data suggest that this high incidence is not leading to increased mortality.
On this there are still contradictory data and it is difficult to know what will happen. The level of uncertainty remains very high. It is true that hospitalisations, ICU admissions and deaths occur with a time lag of a few weeks. The problem is that a much more transmissible variant, even if it is less virulent, does not necessarily mean that it causes fewer deaths: if it grows at such a high rate, if there are many cases in a very short time, there may be more deaths. An intense and rapid sixth wave at issue of cases will lead to a collapse of the health system, which we have already seen has very serious consequences. International health agencies rate status as very high risk. For this reason, some say "prepare for the worst". In this report (15/12/2021) of the ECDC explains the status in Europe.
We do not know if it is more serious, but we also do not know if it will be milder.
Although the issue hospitalisation rate remains low, there is no evidence that Omicron is less virulent than Delta.
Compared to other variants, preliminary results suggest that Omicron multiplies 70 times faster in human bronchi, which may explain why this variant can transmit faster. However, the same study sample found that infection by Omicron in the lung is significantly lower than with the original SARS-CoV-2. This may explain why it results in less severe disease.
Other preliminary work suggests that sera from vaccinated individuals neutralised the Omicron variant at a much lower level than any other variant. However, the same work also suggests that sera from superimmune individuals (those who had been infected and vaccinated or who had been vaccinated and were subsequently infected) were able to neutralise the new variant. Antibodies prevent infection, so this partial escape from the immune response (antibodies) could also influence its increased transmissibility.
What do we do against a variant that is much more transmissible and even more serious?
Against Omicron or any other even more dangerous variant, what we have to do is to remember what we already know... and do it: vaccinations, masks, ventilation, distance, antigen testing, self-confinements, sanitary reinforcement,...
Vaccines work
At the current incidence, if this sixth wave had caught us unvaccinated it would have been a real slaughter. We already saw this with the fifth wave, where the issue of cases increased (then Delta, which was more transmissible, was dominant) but it was not reflected in an increase in deaths as in previous waves. The difference is that most of the most vulnerable older people were already vaccinated. Hopefully something similar will happen now. In three to four weeks we will know.
With the tremendous transmissibility of Omicron, it is likely that many of us will be infected. If you do get infected, it is best if the virus catches you vaccinated. Unprotected people (unvaccinated or previously uninfected) are most at risk. Vaccines are not impenetrable steel armour, you can get infected and you can infect others, albeit less likely. But that does not mean that vaccines are not working. These vaccines are preventing severe cases of the disease, reducing hospital and ICU admissions and reducing mortality. That was their goal. So get vaccinated, not just to protect yourself, but to protect others.
Vaccines induce a powerful immune response. Immunity is much more than antibodies. Antibodies prevent infection and cell-mediated immunity prevents serious disease and mortality. But both are needed. That is why the most vulnerable people need antibodies and cell-mediated immunity, because infection alone can land them in hospital. In older people their immune system also ages (immunosenescence) and they respond less well to vaccine stimuli. It may also happen that the antibody response decreases over time. For this reason, a booster dose, the so-called third dose, may be advisable.
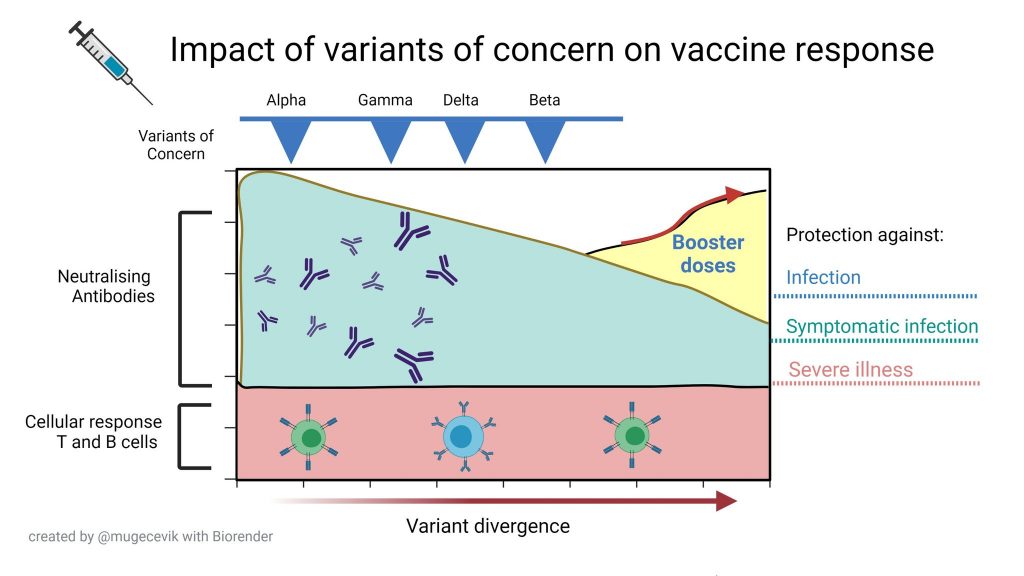
As mentioned above, it appears that the neutralising capacity of vaccine-induced antibodies may be diminished by Omicron. Other work suggests, however, that the cellular response may be able to control the new variant. In any case, several programs of study studies with different vaccines (AstraZeneca, Johson&Johson, Modena, Novavax, Pfizer and Valneca) suggest that a booster dose reduces severe COVID-19 in all age groups and increases neutralising activity against Omicron very significantly.
There is no doubt that the best way to protect against SARS-CoV-2, regardless of the variant, is vaccination. The priority should be: 1) to convince those who have not yet been vaccinated to get vaccinated, and 2) to vaccinate with a third booster dose those who are more vulnerable (elderly, with previous pathologies,...).
Moreover, we must not forget that this is a global pandemic and what happens in South Africa, Peru or India influences us, so vaccines must be provided in those countries where vaccination coverage is still very low fees .
Do we vaccinate children under 12?
This is an extraordinary status , not a normal status . Although cases of severe COVID-19 are very rare in children, this does not mean that there have not been serious cases and even deaths. Clinical trials have shown that vaccines for children aged 5-12 years are safe and effective. In addition, more than 5 million children have been vaccinated in the US and no serious side effects have been reported. Although from an individual point of view one might doubt the need for childhood vaccination, vaccinating children can have other beneficial effects, not only preventive but even therapeutic: it can help reduce the incidence of disease, improve status in schools and reduce the psycho-emotional stress to which children and their families are also subjected. Some argue that vaccinating children to protect the elderly is an aberration, but vaccines have always had that social component: they protect you and they protect others. And I insist, status is not normal at the moment, we are in the midst of a pandemic.
On this point, it is worth remembering that vaccination is not compulsory in Spain. Vaccinating children is a decision that parents must authorise in good conscience. If they have any doubts, they should let their paediatrician advise them. But their decision should be respected and no one should be discriminated against. This sixth wave is NOT the fault of the unvaccinated. The unvaccinated are at greater risk, but they are not to blame for the increased incidence of the virus.
If vaccines are not stopping the virus from circulating, what do we do?
Now is a good time to remember the image of Swiss cheese.
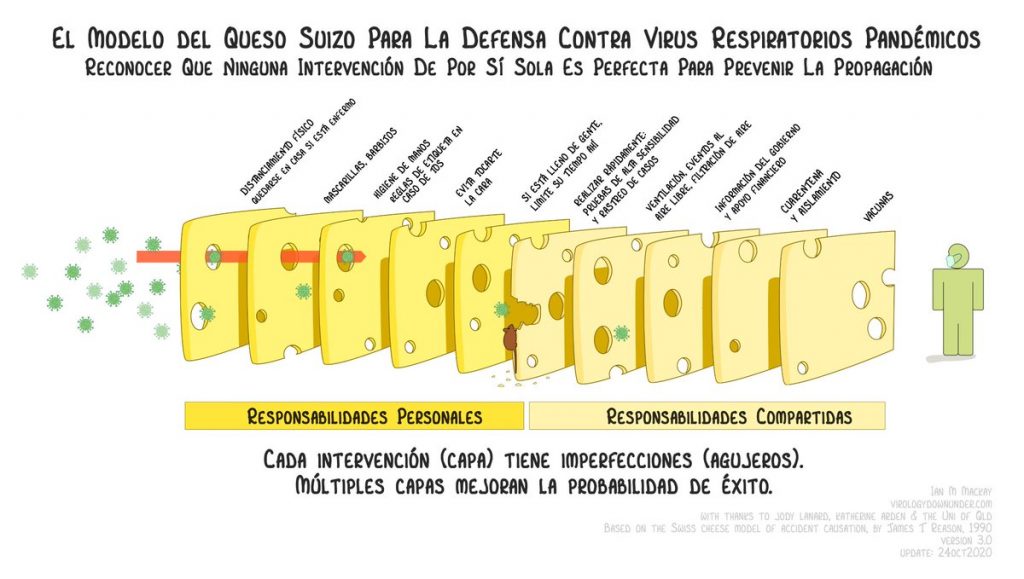
We don't have an impenetrable steel wall to block the virus, not even vaccines. Vaccines are not the only solution, they are part of the solution. No single measure is perfect to prevent the spread of the virus (every layer of cheese has holes in it). But an overlap of measures compensates for individual shortcomings and significantly reduces the risk.
Let us remember that the virus is transmitted by aerosols, like tobacco smoke. Let's imagine a person next to us smoking. Just as tobacco smoke moves around us and we end up breathing it, so will the virus move if we have an infected person next to us. Therefore, a place Closed, poorly ventilated, with many people, talking for a long time and without a mask is the best place to get infected. The masks have result been a super effective measure to prevent contagion.

Masks are necessary indoors and outdoors if there is no safety distance. Outdoors with safety distance the mask is not necessary. The risk of infection outdoors is much lower than indoors. That is one of the reasons why in winter there are more infections of respiratory pathogens, because we spend more time together indoors. It makes no sense, therefore, to close the parks as has been done at other times during the pandemic. All activity is better outdoors than indoors. Going on the street with a mask and taking it off when entering a place Closed is like wearing a helmet on the street and taking it off when riding a motorcycle, because it bothers you to drive.

What does make more sense is to favour indoor CO2 meters. One way to measure the quality of the air we breathe is to measure the concentration of CO2 we expel when we breathe. The higher the concentration of CO2, the greater the amount of air already breathed in by another person. Since we cannot see the virus and cannot measure its concentration in the air, the CO2 measurement is a good indicator. We are more than 20 months into the pandemic, why haven't CO2 meters been installed in enclosed public places?
To improve air quality, cross-ventilation remains essential. If this is not possible, filtration systems can be used. Why haven't air filtration systems been installed in enclosed public places?
Shall we do an antigen test?
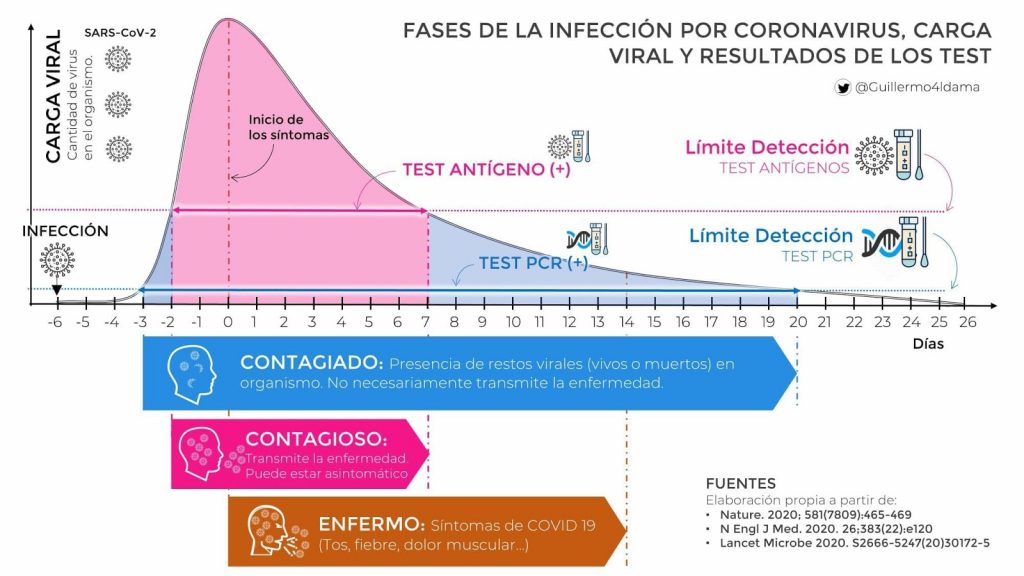
For several months now, antigen tests have been available at available . (You may be interested to read In addition to vaccines, we need antigen tests). When used properly, they can detect people at their most contagious stage. If the test is positive, you should isolate yourself and stay at home. If it is negative, do not relax. There may not yet be sufficient viral load. The best thing to do would be to repeat the test in the following days. In the case of a celebration, it is best to take the test shortly before the event.
These subject tests can be very useful in situations such as the current one where the health system is already collapsing. Why are they not yet sold outside pharmacies, as in other countries? If it is convenient to repeat the test, why are they not cheaper or even distributed free of charge to the population, as in other countries?
Some good news
But there is also good news, albeit very preliminary. For example, the oral drug Paxlovid remains almost 90% effective in preventing hospitalisation and death from COVID-19 in a study of more than 2,200 high-risk patients. Efficacy rises to 94% in those over 65 years of age.
Strengthening the health system is not the citizen's responsibility
This time of year is the season of snot, colds, catarrh, bronchitis, pneumonia, flu... and coronaviruses. Mortality statistics throughout the year (before the pandemic) show that more people always die in winter than in summer, there are hundreds of viruses and bacteria that are transmitted through the air and cause this subject of respiratory problems. It is to be expected, therefore, that every year there will be a peak in incidence and that the health system will be under some strain and a backlog of patients. This winter, in the midst of a global pandemic, the collapse of the system was more than foreseeable. The vast majority of citizens have been obedient, we have complied and have been vaccinated. Whose responsibility is it that the health system is now bursting at the seams? Obviously the virus, but we have been in a pandemic for more than 20 months now. How many doctors/nurses have been recruited? How have screening, diagnostic, primary care and emergency services been strengthened, how many ICU beds have been expanded, why hasn't the legal system been reformed to prevent authorisations being dependent on the decision of a single judge, why do we still have different measures depending on the territory,etc.?
There arepersonal responsibilities (vaccination, use of masks, physical distance, avoiding contagion, avoiding crowded spaces, self-confirmation in the event of symptoms, informing the health service in the event of contagion, complying with quarantines, etc.).) and there are those of the managers (reinforcing the staff of trackers, doctors/nurses, primary care and emergencies, diagnostic laboratories, ICU beds, providing CO2 meters, ventilation and filtration systems, providing and/or facilitating access to antigen testing, adapting legal systems, coordination, effective speech ,...).
All this combination of measures and responsibilities will help us to better control the pandemic, regardless of the current variant. The status is very sensitive, so let's be responsible and take care of ourselves.
This article was originally published in The Conversation. Read the original.
![]()